Featuring
- We Did This Ourselves (poetry)
Carl Bernard Swartz - Democracy on a Razors Edge (essay)
Charles Entrekin - Promising (poetry)
David Radavich - The Mission of Sisyphus (essay)
Editors - The Principles of Quantum Mechanics (poetry)
Jaime Irons - Democracy and Sacrifice (essay)
Luke Wallin - The Old Man in the Plaza (poetry)
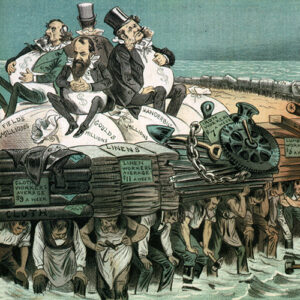
Eugene Berson - The Progressive Impasse (essay)
Demian Entrekin - Sophomores of the Future (poetry)
Richard Rosengarten - The Global Environmental Legacy on the Ohio-Pennsylvania Border (essay)
Eliot Hudson - The Public Lungs (poetry)
Richard Rosengarten - On Collapse… and Renewal (essay)
Matthew Sanderson - For Showers of Meteors and Hours of Rain (poetry)
Jaime Irons - 2027 (Humor)
Aaron Berry - Call for Submissions: Intelligence Issue 10.2